
Male hair loss products fall into a handful of distinct categories, each working through a different mechanism. Understanding those mechanisms helps you evaluate whether a product is likely to work for your situation — and what realistic outcomes look like.
1. Topical Minoxidil
Minoxidil is the most widely used over-the-counter hair loss treatment for men. Originally developed as a blood pressure medication, it was found to promote hair growth as a side effect. Topical minoxidil (2% and 5% formulations) is applied directly to the scalp once or twice daily.
How it works: Minoxidil is a vasodilator — it widens blood vessels and improves circulation to hair follicles. It also extends the anagen (growth) phase of the hair cycle. It does not affect DHT or androgen receptors. This means it addresses the symptom (follicle miniaturization) rather than the cause (DHT sensitivity), which is why it must be used continuously to maintain results.
Evidence: Strong. Multiple randomized controlled trials support its effectiveness for vertex (crown) hair loss in men. Results are more modest for hairline recession. Roughly 60% of men see measurable improvement with consistent use over 6–12 months.
Limitations: Hair regrown with minoxidil is lost within months of stopping. Does not work for everyone. Can cause scalp irritation. Oral minoxidil (by prescription) is increasingly used off-label with stronger systemic effects and different risk profile.
2. Oral Finasteride (Propecia)
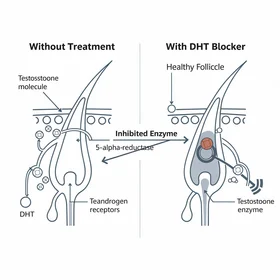
Finasteride is a prescription-only DHT blocker. It works by inhibiting Type 2 5-alpha-reductase, the enzyme that converts testosterone to DHT in the scalp and prostate. Taken daily at 1mg, it reduces scalp DHT by approximately 60%.
Evidence: The strongest of any oral hair loss medication. Multiple Phase III trials showed significant reduction in hair loss and measurable regrowth in the majority of men who used it consistently. Effects are concentrated at the crown and vertex.
Limitations: Requires a prescription. Comes with a documented risk of sexual side effects in a small percentage of men (1–2% in clinical trials, though real-world reports vary). Not suitable for men of reproductive age concerned about fertility. Hair is lost when treatment stops.
3. Natural DHT Blockers (Oral Supplements)
This category covers over-the-counter supplements that inhibit 5-alpha-reductase or reduce DHT activity through natural compounds. Common ingredients include saw palmetto, beta-sitosterol, pumpkin seed oil, pygeum, and green tea extract (EGCG).
How they work: Most work via the same basic mechanism as finasteride — reducing the conversion of testosterone to DHT — but with weaker potency. Saw palmetto in particular has been studied as a mild Type 1 and Type 2 5-AR inhibitor.

Early hair loss typically begins at the temples and crown — the androgen-sensitive zones most affected by DHT.
Evidence: More limited than pharmaceutical options, but several ingredients have small-to-moderate trial support. Products combining multiple DHT-targeting compounds (like Procerin) with a topical component have shown results in IRB-approved studies. Expectations should be calibrated accordingly — slowing loss is more realistic than reversing significant loss.
Advantages: Available without a prescription. Lower side effect profile than finasteride. Can be used long-term as a maintenance approach.
4. Laser Therapy Devices
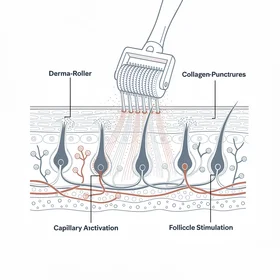
Low-level laser therapy (LLLT) devices — including helmets, caps, and combs — use red light at specific wavelengths (typically 650–670nm) to stimulate follicle activity. They're FDA-cleared for both men and women.
How they work: The proposed mechanism involves photobiomodulation — light energy absorbed by mitochondria in follicle cells increases ATP production and cellular activity. The effect is on follicle metabolism, not on DHT.
Evidence: Several RCTs support modest improvement in hair density and thickness. Results are generally less dramatic than pharmaceutical DHT blockers, and most devices require consistent use (3x per week) to maintain any benefit.
Limitations: Expensive upfront cost ($200–$800+ for quality devices). Requires significant time commitment. Evidence quality is improving but still behind minoxidil and finasteride.
5. Specialty Shampoos and Topicals
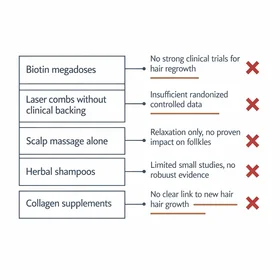
Hair loss shampoos typically contain ketoconazole, caffeine, biotin, saw palmetto, or zinc pyrithione. Most work as adjuncts rather than standalone treatments.
Ketoconazole shampoo has the strongest evidence in this category — it has mild anti-androgenic properties and is shown in some studies to reduce DHT activity at the follicle when used regularly. It's commonly used as a complement to minoxidil or oral DHT blockers.
Caffeine-based topicals have limited but emerging evidence suggesting they may counteract some DHT effects at the follicle level when used consistently.
Biotin supplements are widely marketed for hair but primarily address deficiency — if your biotin levels are normal, supplementing is unlikely to produce results.
How to Choose: A Step-by-Step Process
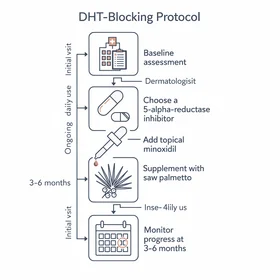
Getting started with a male hair loss product can feel overwhelming given the number of options. Here's a practical process for making an informed decision:
- Confirm your diagnosis. Make sure your hair loss is androgenetic alopecia (DHT-driven pattern loss) rather than another condition like alopecia areata or telogen effluvium. A dermatologist can confirm this in one visit.
- Determine your Norwood stage. Identify whether you're at early (I-III), moderate (III-IV), or advanced (V+) loss. This determines which product categories are most relevant.
- Decide your risk tolerance. Are you comfortable with prescription medications and their potential side effects? Or do you prefer starting with natural, non-prescription options? Both paths have clinical support.
- Start with one product category. Don't try everything at once. Pick a DHT blocker or minoxidil as your foundation and use it consistently for at least 90 days.
- Evaluate objectively. Compare dated photos, not daily mirror impressions. Look for reduced shedding first (month 2-3), then gradual thickening (months 4-6).
- Add or adjust at 6 months. If your initial choice isn't producing sufficient results, consider adding a complementary product (e.g., adding minoxidil to a DHT blocker) rather than abandoning your current approach.
Alternatives to Traditional Hair Loss Products
Not every man wants to commit to daily topicals or oral supplements. Here are other options to consider instead of conventional male hair loss products:
- PRP (platelet-rich plasma) therapy — A clinic-based alternative using concentrated growth factors from your own blood. No daily maintenance, but requires recurring appointments and costs $500-2,000 per session.
- Hair transplant surgery — The only permanent solution for restoring hair in bald areas. Modern FUE techniques produce natural results, but it's an alternative best suited for stabilized loss at Norwood IV+. Cost: $4,000-15,000+.
- Scalp micropigmentation — A cosmetic tattoo alternative that creates the appearance of a close-cropped hairstyle. No medical intervention required. Results last 3-5 years before touch-ups.
- Hair fibers and concealers — Keratin fibers (like Toppik) that bond to existing hair for immediate cosmetic improvement. A non-medical alternative that works alongside — or instead of — treatment products.
- Acceptance — A growing number of men choose to embrace hair loss rather than treat it. This is a legitimate alternative with zero cost, zero side effects, and zero daily maintenance.
Choosing the Right Category
No single product works for everyone. The most important variables are: how early you start, how aggressive your loss pattern is, and whether you prefer pharmaceutical or natural approaches. Many men use a combination — for example, a natural DHT-blocking supplement alongside minoxidil and a ketoconazole shampoo.